
 Communicate:
Communicate:
Advocate: Ensure that physicians have the necessary resources to do their job properly and safely: personal protective equipment, regularly updated policies and protocols, and staff support.
Provide personal support: Ensure that physicians have access to resources, such as child care while kids are out of school, grocery shopping, walking pets, so that they can be at work or recover from work.
Ensure emotional support and counseling: Organize multiple sources of support for physicians, including access to online mindfulness, yoga, and cognitive behavioural therapy sessions; peer support programs and groups; access to family physicians for self-care; access to psychologists and psychiatrists for assessment, counseling, and medical treatment.
Lead self: Monitor your own psychological reactions and responses to ensure effective self-care; maintain your own physical health by taking appropriate precautions.
Maintain humour: Humour facilitates divergent thinking leading to creativity and viable solutions, while a somber mood leads to convergent thinking and blocked vision.
Keep your sense of purpose: Maintain your vow to care and to get your team, yourself, and Canada out of this chaotic state and through the pandemic.
If you have time, please also read the following pages which explain the difference between complex systems (such as the health care system with which physicians are familiar) and chaotic systems (in which physicians are not used to working) and the different leadership styles needed. Below, we summarize the literature and provide a simple explanation of the Cynefin framework, which is being applied by several Canadian health organizations in the context of COVID-19. It is also part of the PLI course on Social Complexity.
 The Cynefin framework
The Cynefin framework
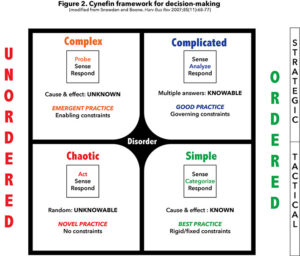
The COVID-19 crisis has quickly changed all our systems, including health care, the economy, finance, education, and supply chains, from complex to chaotic. Chaotic systems require agility to navigate a wide range of leadership styles from “command and control” to “distributive,” and everything in between. Physicians have been trained as experts, meaning that they are very good at making decisions in the ordered world. The Cynefin framework (Figure 2) describes four systems — simple, complicated, complex, and chaotic — and the leadership styles needed in each case, including the COVID-19 crisis.
In simple systems (lower right quadrant), there is a high degree of evidence-informed certainty about what needs to be done and a high level of agreement among all stakeholders. The cause-and-effect relationship is well known and decisions are made and agreed on based on best practice. An example would be the execution of a protocol for a specific condition. In such a simple system, one senses (observes, measures), then categorizes what is observed, and makes the appropriate response.
Complicated issues (upper right quadrant) require groups of experts. For example, when a patient with multiple comorbidities needs cancer surgery, several specialists must do the sensing, each in their own field of expertise, then analyze as a team and respond with one of multiple possible answers, resulting in good practice. As physicians, we are comfortable and skilled at working in the ordered world, dealing with one patient at a time.
We are less comfortable in the unordered world (Figure 2, left side), where there is less evidence and agreement on how to do things. Under normal conditions, the health care system is complex (upper left quadrant) and in constant flux because of the many moving elements with many known and unknown interactions. Because there is no clear relationship between cause and effect, we understand why things happen only in retrospect. As a result, there is no best practice, only emergent practice that can be tested and adjusted based on ongoing sensing (measuring) and learning. In complex systems, leaders probe first, perhaps by doing a small pilot trial, sense by observing what the emerging patterns might be, and then respond by amplifying or damping the returning signal or launching a different probe. In complex systems, we often have some luxury of waiting while we sense.
In a chaotic system (lower left quadrant), there is little time to act, particularly in a crisis situation, such as that precipitated by COVID-19. Overall randomness makes the relationship between cause and effect unknowable. Because of the lack of patterns and system constraints, a leader must act quickly to (hopefully) “stop the bleeding.” The leader then senses what is happening in the system, where any type of pattern or stability might be present, or where it might be absent. Finally, a response will try to move the system from chaotic to complex. Because of all the randomness and the unknowable, practice is novel.